Case 32
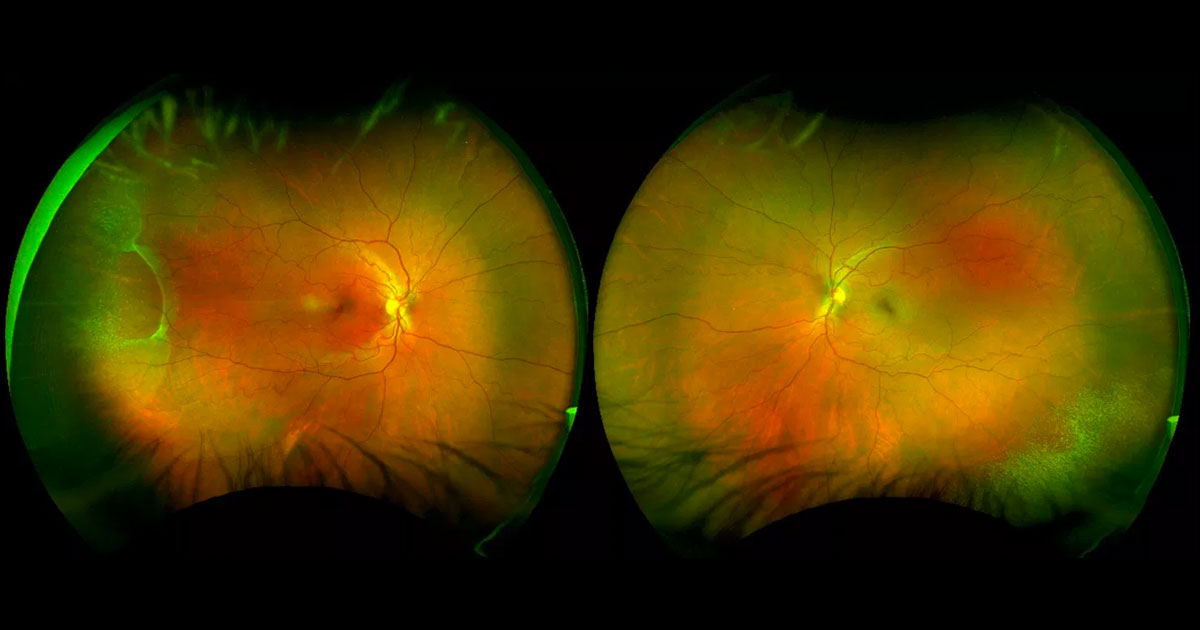
Figure 1. Colour photograph demonstrating an area of elevation in the right far temporal retina, with a fine white speckled appearance surrounding this as well as in the left inferotemporal periphery.
Author and Editor: Adrian Fung
A 43-year-old female was referred with a possible right retinal detachment.
Case history
A 43-year-old female was referred by her optometrist complaining of a one-month history of flashes and floaters in her right eye. She also complained of headaches starting that day. The optometrist was concerned she had rhegmatogenous retinal detachment. There was no previous ophthalmic history nor any relevant medical history.
Visual acuity was 6/9.5+2 ph 6/4.8-1 in the right eye (OD) and 6/6 in the left eye (OS). Intraocular pressures were 21mmHg (OD) and 19mmHg (OS). Anterior segment examination was normal and there was no vitreous pigmentation. On fundus examination there was an area of elevation between the 8 and 10 o’clock meridia in the righ eye with a fine white speckled appearance (Figure 1). A similar fine white speckled appearance was detected in the left inferotemporal periphery, but without any elevation. Both maculae and optic nerves were normal. The posterior hyaloids were still attached.
What is your diagnosis?
Click to reveal answer
Differential diagnosis
The differential diagnosis for a peripheral retinal elevation includes:
- Retinal detachment
- Rhegmatogenous (with a break)
- Serous/Exudative
- Tractional
- Rhegmatogenous (with a break)
- Peripheral senile (degenerative) retinoschisis
- Choroidal detachment
- Pars plana cyst
Additional history, examination and investigations
Optical coherence tomography (OCT) through the right temporal retinal periphery demonstrated a split in the retina (Figure 2). The thicker outer retina had a rolled edge at the margin of a large outer retinal hole. Scleral indentation was performed with indirect ophthalmoscopy and no inner retinal break was identified.

Figure 2. Optical coherence tomography of the far peripheral retinal periphery. There is splitting of the retina into two layers. The thicker outer retina has a rolled edge at the margin of an outer retinal hole (thick arrow), whilst the thinner inner retina continues above this (thin arrow). Artefactual reflections of the inner retinal layer and retinal pigment epithelium are marked by asterixes.
DIAGNOSIS
Senile (degenerative) retinoschisis with larger outer retinal hole and associated snowflake degeneration.
Clinical course
Given the new onset of symptoms, a follow-up visit was arranged for six weeks. The patient was advised to represent immediately if they developed symptoms of retinal detachment including an increase in photopsiae, floaters and/or peripheral scotoma.
Discussion
Peripheral senile (degenerative) retinoschisis is a common condition affecting 7% of the population over 40 years of age.(1) Two forms have been described histologically: “typical” (flat)(2) and “reticular” (bullous)(2). The split in the “typical” form occurs in the outer plexiform layer, whilst the split in the “reticular” form occurs in the nerve fibre layer. Most cases are asymptomatic, although peripheral absolute scotomas may be noticed. Differences between senile (degenerative) retinoschisis and rhegmatogenous detachment include:
- More common in hypermmetropes (versus myopes)
- Usually asymptomatic
- No vitreous cells
- Commonly bilateral, inferotemporal and anterior
- Usually convex, smooth, thin retina that moves in unison with scleral indentation
- No full-thickness retinal tear
- No proliferative vitreoretinopathy
The vast majority of senile (degenerative) retinoschisis do not require treatment. Outer layer breaks (OLB) are common, and have been found in 10%(4) to 27%(5) of all cases. Localised detachment of the outer retinal layer (“schisis-detachment”) can occur but do not require treatment.(4) Rarely, progressive symptomatic rhegmatogenous retinal detachment complicating retinoschisis (PSRDCR) can develop. Estimates of incidence lie between 0.009%(6) and 0.05%(7) of all senile (degenerative) retinoschisis. This usually occurs when there is development of small inner retinal breaks in addition to larger outer retinal holes, allowing for a conduit for vitreous fluid to enter the subretinal space. The most common time for this to occur is during development of posterior vitreous detachment.
Most cases of PSRDCR can be managed by scleral buckling and cryopexy.(8) If the breaks are too posterior, pars plana vitrectomy has been successfully described.(9,10)
TAKE HOME POINTS
- Senile (degenerative) retinoschisis is a common condition where there is splitting of the peripheral retina.
- Most cases are asymptomatic and do not require treatment.
- Rarely, a progressive symptomatic rhegmatogenous retinal detachment can develop. This is usually treatable with a scleral buckle.
REFERENCES